Founded in 1299, Malta’s Santo Spirito Hospital was more than 200 years old when the Knights Hospitalier arrived on the island and decided a new hospital was needed. Arpan Banerjee tells the story of a hospital ahead of its time.
The Knights Hospitalier were a proud military order of the Catholic Church founded in the 11th century to fight as a military force in the Crusades and also take care of the sick. After the fall of Jerusalem, they eventually migrated to Malta in 1530 where they stayed and ruled the islands until 1798 when they were defeated by Napoleon Bonaparte.

Sacra Infermeria today: author’s photo
At the time of their arrival, Santo Spirito Hospital was the country’s main hospital, but it was outside Rabat, some distance from Valletta. The Knights Hospitaliers felt a hospital was required in Valletta, now the capital of Malta, and in 1574 they built the Sacra Infermeria or Holy Infirmary, at the northern tip of the small promontory of land surrounded by the Grand Harbour. It became one of the leading hospitals in Europe.
A modern hospital
The Sacra Infermeria Hospital had around 500 beds, but could expand to accommodate almost 900 patients if needed. Although not called such then, the Nightingale-style wards included one of the largest halls of its time. The Old Ward, as it was known, was more than 150 metres long. A small ward served the dying. In the basement was a 100-bedded ward for wounded or sick soldiers and sailors. The hospital treated not only the sick but also provided accommodation to those on pilgrimage to the Holy Land. What made the hospital unique, however, were the facilities, the most modern of the time, and high standards of care long before Florence Nightingale made known the importance of nursing.
In the seventeenth century, the hospital boasted a school of anatomy and surgery founded by the Grand Master Cotoner. Cadaveric dissection took place, which did not become a routine part of medical training until the eighteenth century and beyond in Britain. In addition, Sacra Infermeria had a wing for patients with infectious diseases and a ward for the mentally ill patients.
 After the brief rule of Malta by the French, the British took over in 1800, and the hospital became an important base for wounded soldiers, as well as the local sick. It played an important role in the Crimean War and First World War due to its strategic position in the Mediterranean, south of Sicily, and known as the Station Hospital.
After the brief rule of Malta by the French, the British took over in 1800, and the hospital became an important base for wounded soldiers, as well as the local sick. It played an important role in the Crimean War and First World War due to its strategic position in the Mediterranean, south of Sicily, and known as the Station Hospital.

The Great Ward of the Station Hospital, Malta c 1906, public domain
The hospital was decommissioned in 1918 after WW1 ended. In WW2, the hospital building survived partial bombing, and after the war it served briefly as a base for the Allied troops based in Malta. The Maltese police then took over the site. A new general hospital was commissioned in Malta in the 1920s, St Luke’s Hospital outside Valletta, and this was replaced by the current teaching hospital Mater Dei in 2007.
Today the old building of the Sacra Infermeria has been renovated internally and converted into a conference centre. The Great Hall survives and is a reminder of the hospital’s illustrious past and important place in medical history. The Knights of St John no longer rule Malta but exist as the Sovereign Military Order of Malta (SMOM) and perform a global humanitarian role and charitable work . The St John Ambulance that operates in Malta is a direct legacy of this order.
Dr Arpan Banerjee is a retired consultant radiologist from Birmingham. He is currently the Chairman of the International Society for the History of Radiology and a past Chairman of the British Society for the History of Radiology. His latest book project was co-editing and contributing to the Pioneers in Radiology Worldwide at the time of Wilhelm Conrad Röntgen.
References
https://en.wikipedia.org/wiki/Mediterranean_Conference_Centre
Mediterranean Conference Centre
https://whc.unesco.org/en/list/131/ City of Valletta
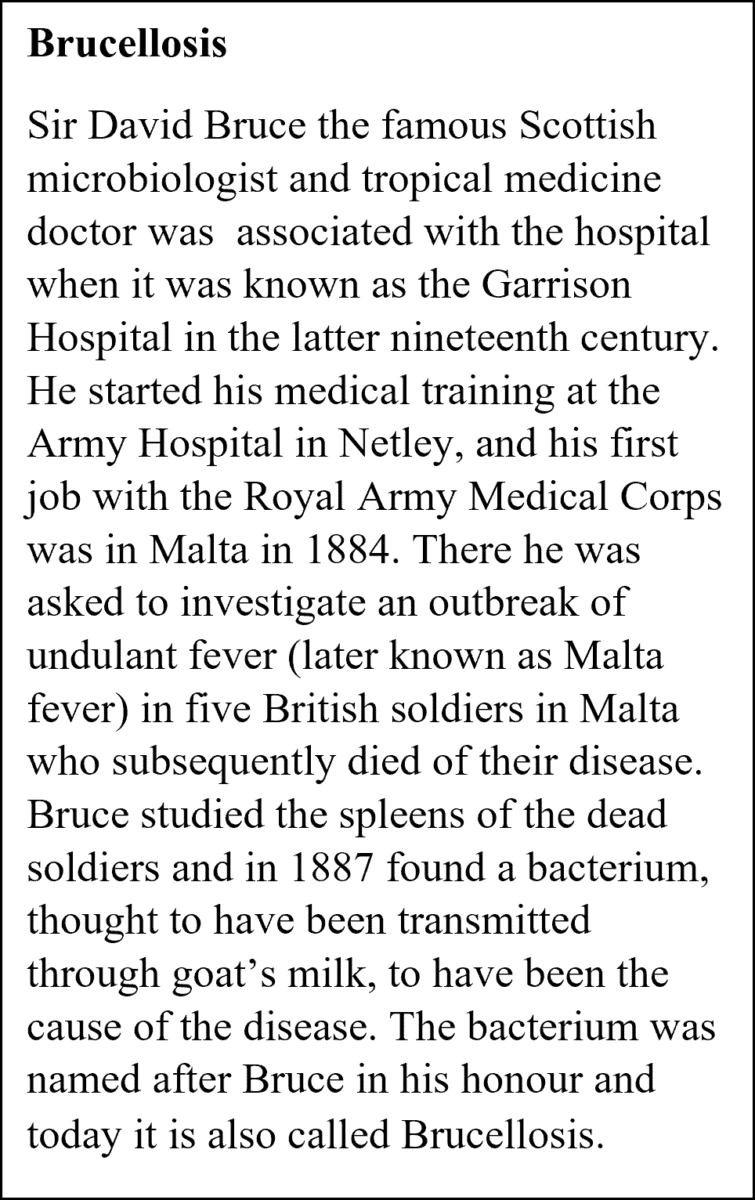
Major-General Sir David Bruce, K.C.B., F.R.S. Nature 129, 84–86 (1932). https://doi.org/10.1038/129084a0