Dora Challis Colebrook (1884 – 1965) has, in my opinion, been overlooked as the architect of the first randomised controlled trial (RCT) in Britain, says Martin Edwards.
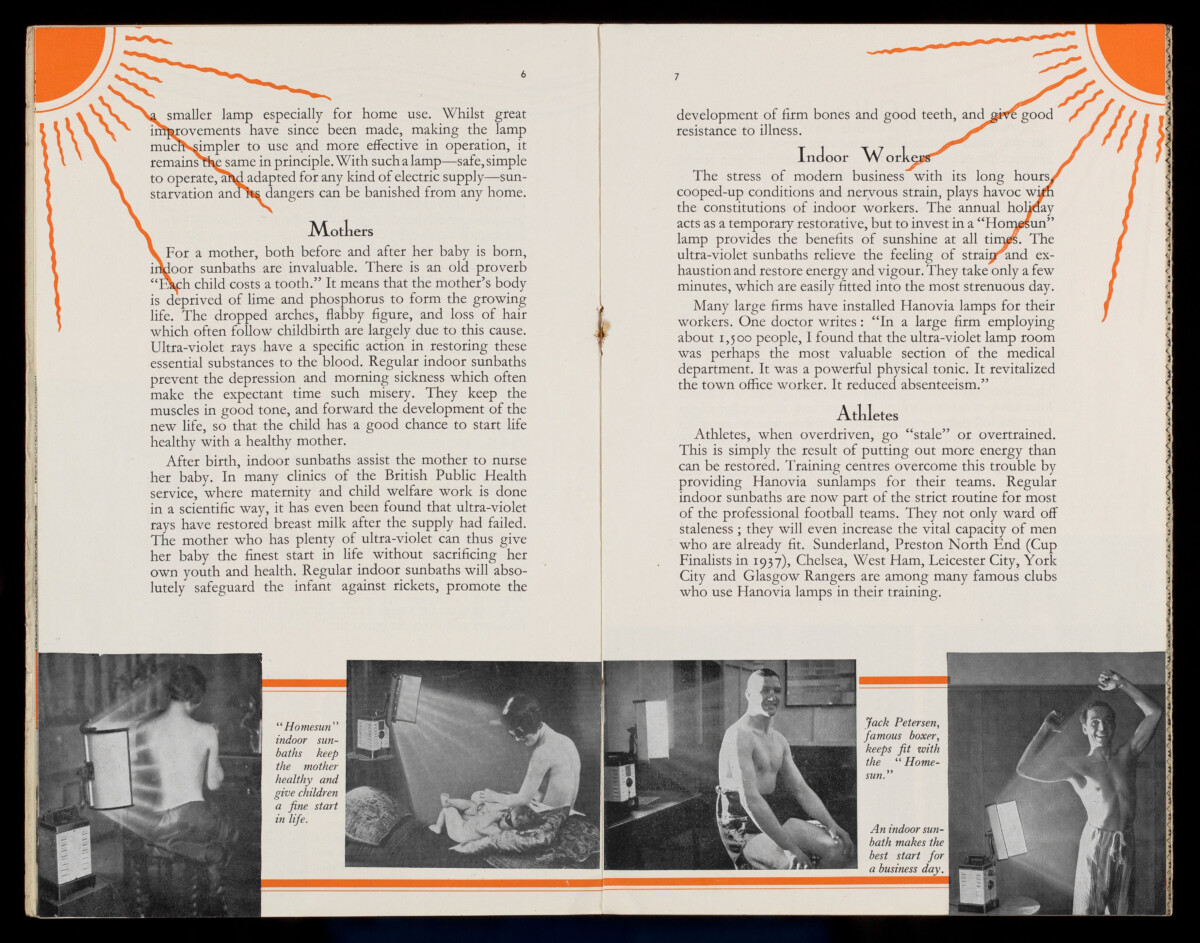
The trial in question concerned light therapy. The 1920s saw a ‘boom’ in enthusiasm for treating all manner of medical conditions with bright light, particularly ultraviolet (UV). Hospitals all around Britain opened light therapy departments, private doctors offered the treatment and manufacturers sold units for the public to use at home. Britain’s dull, smog-congested cities were thought to render its inhabitants particularly suitable for light therapy, which rapidly became regarded as a panacea.
Promoting light therapy
The Medical Research Council (MRC), created in 1911 as the Medical Research Committee, was at this time attempting to position itself as the only organisation properly able to test therapeutic efficacy. The explosion of light therapy caught the MRC on the hop. Eager to evaluate the treatment before its popularity made its opinion irrelevant, the MRC sought a worker in the field. Thanks to an influential MRC member, the bacteriologist Leonard Colebrook (1883 – 1967), they lighted upon Dora Colebrook – Leonard’s sister.
Dora was a doctor, trained at the Royal Free Hospital in London. After a stint as a gynaecologist in Sheffield and some years in Cambridge as a GP, she worked in an infant welfare centre in Islington administering light therapy to physically feeble children. Asked in 1925 by Walter Morley Fletcher, the MRC Chair, to summarise her experience she described an ‘almost monotonous’ increase in liveliness, vigour, weight gain and general wellbeing among the children she treated. Fletcher asked her to submit a research proposal. Inexperienced in research, Colebrook initially offered a hopelessly ambitious scheme which Fletcher rejected. There followed one or more conversations with someone unspecified from the MRC, and Colebrook submitted a revised proposal for a study which she performed in 1927.
The trial
Colebrook randomly divided 300 children ‘by drawing lots’ into three groups. One received UV therapy, the second ‘sham’ therapy from a lamp screened by UV-excluding glass, and the third was untreated. Colebrook recorded the children’s heights, weights, incidence of infections, school absences and subjective impressions from teachers, parents and herself. Her results were unequivocally negative, demonstrating no apparent benefit of light treatment, and were published in an MRC special report in 1929.[1]
The response was immediate and vitriolic. Doctors, unqualified light therapy practitioners, manufacturers and the public joined in the vilification of Dora, referring to her in medical journals and lay newspapers in isolation, implying that she was a lone maverick researcher, without reference to the MRC. Her gender was repeatedly stressed, the Daily Telegraph describing her simply as ‘a woman writer.’ Dora faced equal vitriol in person at medical meetings where her findings were dismissed with frank disbelief, doctors preferring the subjective opinion of more distinguished medical figures. Eventually the furore fizzled out; Dora went on to work with her brother Leonard on antibacterial therapy, and her light study, something of an embarrassment to the MRC due to its reception, was quietly forgotten.
This was a clash of epistemologies; a new ‘scientific’ therapeutic assessment versus the traditional wisdom and experience of experts. But Dora was sidelined, not simply because she was presenting an unexpected and unpopular finding, but because her relatively lowly status in the medical hierarchy, and her gender, enabled opponents to single her out for opprobrium.
Her study is arguably the first true RCT in this country. Yet when the MRC chose an exemplar to promote the RCT as its own invention, it employed the streptomycin trial of 1948 – a popular trial of a supposed ‘wonder drug’ which provided the positive results that everybody wanted and expected. Had Dora’s critics been more amenable to evidence, and the MRC less embarrassed by her reception, hers might have been recognised as the first true RCT.
Martin Edwards worked for more than 30 years as a GP in South London while pursuing an interest in history of medicine, gaining an MSc in history of science and medicine at Imperial College in 1998 and an MD in history of medicine from UCL in 2004. His interests include the evaluation of therapeutic efficacy and therapeutic bedrest in the 19th century.
[1] D. Colebrook, Irradiation and Health (London: HMSO, 1929).
Extracts of the report: https://www.jameslindlibrary.org/colebrook-d-1929/