
In about 1841, Belgian doctor Constantin Pierre Crommelinck toured various psychiatric institutions in England, France, and Germany. His report reviewed not just various English asylums and also the training of English doctors. Peter Carpenter recounts his none too flattering findings.
Constantin Pierre Crommelinck (1814-1884) was the son of a Belgium surgeon who trained as a doctor and became a teacher of anatomy at the École de Médecine in Bruges. He initially had some success as a surgeon, but then turned to psychology and psychiatry. There is no official biography for Crommelinck, but his entry in Dutch in Wikipedia indicates he was not an easy colleague.
In about 1841, he toured various psychiatric institutions in Belgium, France, England and Germany and also investigated the training of English doctors. The following year, he reported his findings to the Belgian Minister of the Interior Jean-Baptiste Nothomb: Rapport sur les hospices d’aliénés de l’Angleterre, de la France, et de l’Allemagne. (A report on asylums of England, France and Germany, 1842).
In this report, he made recommendation for the design and therapeutic organisation of future Belgian asylums. His descriptions of various asylums in England are little known in the UK, other than that of Gloucester Asylum, which appears in several biographies of Samuel Hitch, the founder of the first British psychiatric association in 1841.
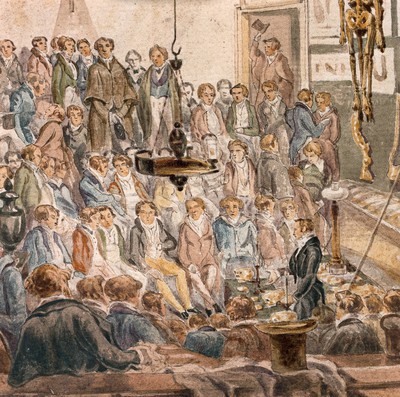
Hunterian anatomy school, London, 1839 by R. B. Schnebbelie, Wellcome Collection
English medical education mocked
In the same report, Crommelinck took the opportunity to make very pointed remarks on the English medical profession and medical education. While commenting on the richness of England’s material resources, he mocked the surgeons’ habit of having an apprenticeship and then attending a selection of classes in London. He wrote:
“At the end of three years’ training with a physician or surgeon, where the pupil has learned (and how else?) physiology before anatomy, therapeutics before pathology, and practice before anything else, he goes back to school, … spends two years there, and qualifies as a physician or surgeon-apothecary. These two years pass like the other three, with the only difference that all the branches are no longer taught by one and the same individual, but by five or six, all teaching pell-mell, without troubling themselves about each other or prescribing to their disciple any order to follow. …Thus the pupil begins, and attends pell-mell, lessons in physiology, anatomy, therapeutics, pathology, medical and surgical clinics, childbirth, etc.
Having attended lessons from each teacher, Crommelinck then went on to describe the anatomy lesson as the most absurd, ridiculous and contrary to common sense. “I will cite among others the one that Mr. Macmurdson gave at St. Thomas Hospital. It was the tenth since the opening of his course; it related to the mucous membranes: all the students, with two or three exceptions, were true beginners. Fifty jars containing different pathological or monstrous alterations of the mucous membranes were placed on the table.
“Mr. Macmurdson took a notebook from his pocket and, using his finger to mark his place, began to read very fast a long, profound and learned dissertation on the past, present and future, healthy and sick, natural and monstrous state of the mucous membranes in man as in other animals. The most scabrous questions of theory and practice were discussed in this reading; he talked about typhus, inflammation, cancer, tumours haemorrhage, bleeding, leeches, calluses, strictures, astringents, styptics, molluscs, pachyderms, mammals, Peyer’s glands, Brunner’s glands – do I know what a jumble of absurdities did not come out of his mouth, while seriously begging his students to pay scrupulous attention to the elementary principles that were going to develop before them?”
[Pages 69-71, Peter Carpenter’s translation]
Rather than pretending to listen and understand, wrote Crommelinck, the students had fun cutting figures in the benches, whispering among themselves and kicking each other. They “ended the farce by applauding excessively when the hour of freedom arrived.”
The lecturer compared with Molière’s comedic doctor from the play Le malade imaginaire, was probably Gilbert MacMurdo, a surgeon at St Thomas’s in the 1846 Medical Directory. It is surprising that Crommelinck named an individual, but the early signs of irascibility seem to have ripened into vitriol later in his career.
Peter Carpenter is a retired psychiatrist who researches the history of UK mental health institutions.
Further reading:
Rapport sur les hospices d’aliénés de l’Angleterre, de la France, et de l’Allemagne is available at the Wellcome Library and the library of the Royal College of Psychiatrists. Digital copies can be found by internet search.






